
In several publications of this page I have presented patients of different ages, different gender and different pathologies of the temporomandibular joints.
This is the second case report about a patient with prosthetic protocols built on implants.
I call once again the importance of the attention in the diagnosis of temporomandibular joints pathologies and mandibular position as a key part of any procedure in dentistry.

Female patient 54 years old arrived to the clinic for consultation with severe headache complaints, pain in the temporomandibular joints, pain in the cervical spine, sore shoulders, ear pain, feeling of clogged ears and crepitation in both temporomandibular joints.

The patient was referred by her dentist who performed the treatment of implants and prosthetics, rehabilitating the patient, but without being able to relieve the pain that afflicted her.

Part of the questionnaire completed by the patient.
The patient reports daily pain.
FUNCTIONS THAT AGGRAVATE HER PAIN:
Mastication
Opening the mouth
Laughing
Yawning
The patient also refers back pain and numbness and tingling in the arms and fingers.
Refers that she wakes up with body aches.

Patient habitual occlusion on the day of consultation.
The patient had fixed prostheses supported on implants on the lower jaw and a removable upper protocol supported on implants on the maxilla.
 Patient’s superior and inferior oclusal view of the prostheses supported on implants on the day of consultation.
Patient’s superior and inferior oclusal view of the prostheses supported on implants on the day of consultation.

Image of the oral cavity of the patient without the upper prosthesis.

Patient’s superior and inferior oclusal view without the superior prostheses.

Patient’s initial panoramic radiograph before treatment with the prosthesis in the habitual occlusion before treatment.
Presence of 4 metallic implants in the maxilla 2 on the right side and 2 on the left side; and 5 implants in the anterior mandible region.
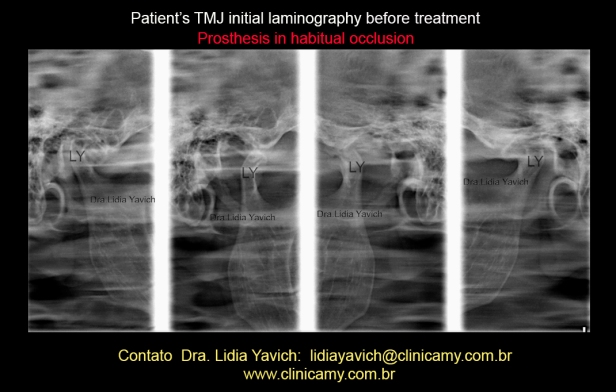
Patient’s TMJ right and left laminography, closed and open mouth: posterior positioning of the articular processes in the joint cavities when the jaw is in maximum intercuspation position.

Patient’s lateral radiograph with prosthesis in habitual occlusion.

Patient’s lateral radiograph and cervical spine with prosthesis in habitual occlusion before treatment.
Alterations of the cervical spine, loss of physiological lordosis and loss of intervertebral spaces especially between the vertebrae C4, C5 and C6.
Ricketts cephalometric analysis before treatment with prostheses in habitual occlusion.

Values of point A convexity and lower facial height before treatment.
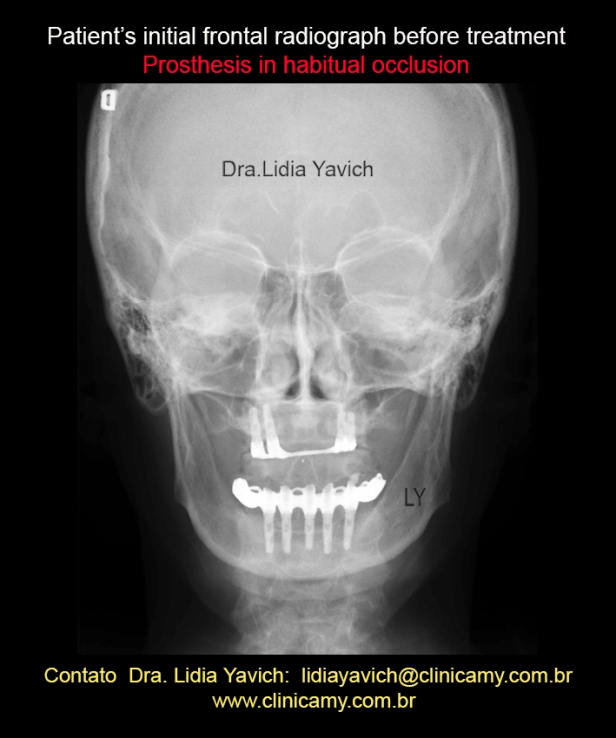
Frontal radiograph of the patient with the prosthesis in habitual occlusion.

MRI, sagittal slice of the right TMJ closed mouth: there is an irregularity of contour with reduction of the superior aspect of the mandibular condyle, the condyle is ante versioned. There is a small anterior osteophyte.
The articular disc is displaced anteriorly, WITHOUT REDUCTION when the mouth opens.
Presence of subcortical bone cysts in the anterior superior aspect of the mandibular condyle.
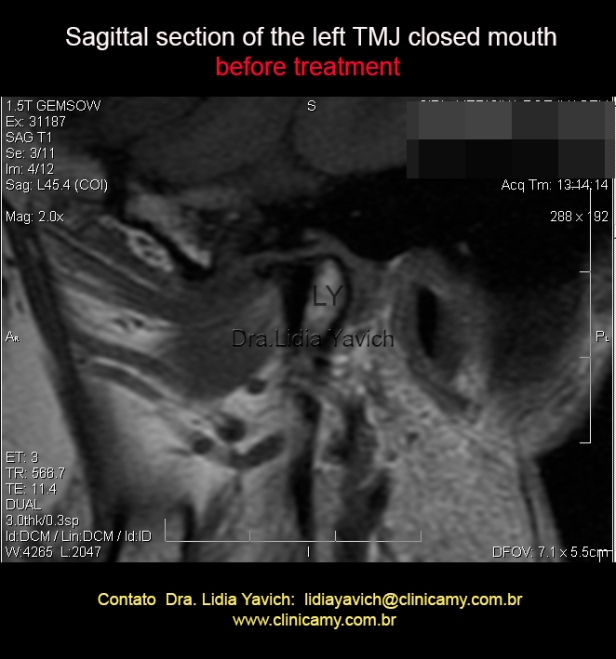
MRI, sagittal slice of the left TMJ closed mouth: there is a substantial irregularity of contour of the upper portion of the mandibular condyle, with the formation of an anterior osteophyte.
There is a rectification of the articular eminence.
The disc has reduced dimensions lying anteriorly displaced WITHOUT REDUCTION when the mouth opens.
Can be seen an important hipossinal compatible with avascular necrosis.

MRI, another sagittal slice of the left TMJ closed mouth: there is an important irregularity of contour of the superior aspect of the mandibular condyle and a formation of an anterior osteophyte.
There is a rectification of the articular eminence.
The disc has reduced dimensions lying anteriorly displaced WITHOUT REDUCTION when the mouth opens.
Can be seen an important hipossinal compatible with avascular necrosis.

MRI in T2 clearly shows the joint effusion.
The differential diagnosis of TMJ effusion has a broad spectrum as the effusions in other joints in other parts of the skeleton.
MRI (magnetic resonance imaging) can give us a lot of information, not just the disc position.

MRI, frontal section of the right and left TMJ, closed mouth. Upper lesion in the right mandibular condyle, as described in the same sagittal slice of the same condyle as subcortical bone cysts.
In the slice of the mandibular head on the left side can be seen an important hipossinal compatible with avascular necrosis.
Avascular necrosis occurs when blood flow to a bone is interrupted or reduced. It can be caused by various conditions, such as bone or joint damage, pressure inside the bone and other medical conditions.
The condyle affected by avascular necrosis has low signal on T1-weighted images as a result of edematous changes in trabecular bone.

Sagittal sections of the right TMJ, closed mouth before the treatment.
There were previously posted to highlight the images I find most relevant, but also this series are registered.

MRI,sagittal sections of the right TMJ, open mouth before the treatment. There is a limitation on opening of the mandibular condyle.

MRI, sagittal sections of the left TMJ, closed mouth before the treatment.
There were previously posted to highlight the images I find most relevant, but also this series are registered.

MRI,sagittal sections of the left TMJ, open mouth before the treatment. There is a limitation on opening of the mandibular condyle.
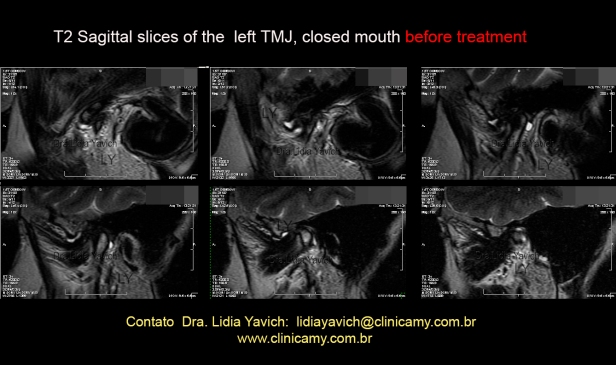
MRI, T2 sagittal sections of the left TMJ, closed mouth before the treatment.
There were previously posted to highlight the image I find most relevant, but also this series are registered.
Serial in T2 clearly showing the joint effusion.
Tests were done on the patient to investigate systemic inflammatory disease, which were all negative.
It was also investigated chlamydia trachomatis infections, mycoplasma pneumoniae infections and beta hemolytic streptococcus infections , results in this case were also negative.
It was also investigated the functioning of the thyroid.

The masticatory muscles of the patient were electronically deprogrammed and DIO (intraoral device) was constructed in neurophysiological position. In other publications computerized kinesiographic methods were mentioned.
In occlusion most often the healthy or pathological condition of the inter-oclusal space is not objectively considered. In this case the free space of the pathological patient is almost 7 mm and a retro position 0 8 mm.

With this data and ALWAYS WITH THE INFORMATION OF IMAGES, we built a DIO (intraoral device) to keep the three-dimensionally recorded position.
This device must be tested electromyographically to objectively measure the patient.

It is essential to control the DIO (intra oral device) as the patient is treated and the mandible is repositioned.
In this case the control still shows us the need for recalibration of the DIO (intraoral device)

Comparative panoramic radiographs: before treatment and after neurophysiological treatment.

Patient’s frontal radiographs comparison: with the prosthesis in habitual occlusion and the DIO intraoral device built on the prosthesis.

Right and left temporomandibular joints laminographies, closed and open mouth comparison: with the prosthesis in habitual occlusion and with the DIO intraoral device built on the prosthesis.

Ricketts cephalometric analysis after treatment with the DIO constructed on the prostheses in neurophysiological occlusion.

Values of point A convexity and lower facial height after treatment.

Patient’s lateral radiographs comparison: with the prosthesis in habitual occlusion and with the DIO built on the prosthesis in neurophysiological position.
The DIO (intra oral device) is used to support, align and correct deformities in order to improve the functions of the jaw, temporomandibular joints and the muscles that move both. This device should be checked and recalibrated as the records indicate the need for modification.

Comparison of aesthetic Ricketts plane in lateral radiograph with prosthesis in habitual occlusion and the DIO constructed on the prosthesis in neurophysiological position.

Comparison of T1-weighted images: before treatment and after treatment: we can see the improvement in medullary signal.
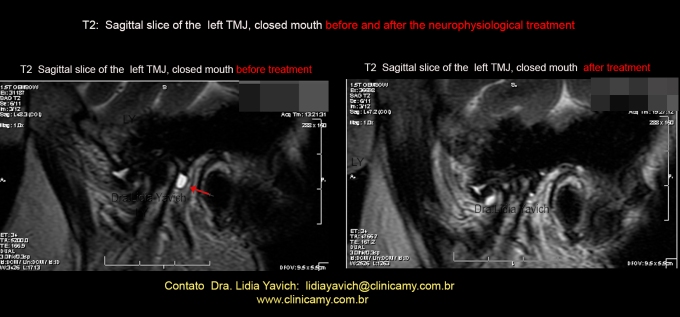
Comparison of T2-weighted images: before and after treatment. It is clear in the first image the inflammatory signal and in the other image the improvement of the intramedullary signal and the remission of posterior effusion.

Comparison of T1-weighted images: before treatment and after treatment, we can see the improvement in medullary signal and improvement of the cortical bone.

Frontal T1-weighted images comparison, before and after treatment treatment: we can see the improvement of the upper lesion on the right mandibular condyle.

Frontal T1-weighted images comparison, before and after treatment: we can see the improvement in medullary signal and improvement of the cortical bone of the left mandibular condyle.

Comparative sagittal sections of the right TMJ open mouth, before and after treatment.
Notice the mandibular condyles WITHOUT LIMITATION IN OPENING in relation to the limitation that had before treatment.

Comparative sagittal sections of the left TMJ open mouth, before and after treatment.
Notice the mandibular condyles WITHOUT LIMITATION IN OPENING in relation to the limitation that had before treatment.

Patient’s postural frontal comparative images before and after treatment.

Patient’s postural profile comparative images before and after treatment.

Ricketts cephalometric analysis before and after neurophysiological treatment.

Skeletal problems in Ricketts cephalometric analysis before and after treatment.

“Headache (already when waking up in the morning), tiredness sensation at the cheekbones, strong tensing at the shoulders and neck, “clicks” at the temporomandibular joint, ear pain… consequently I also felt irritation, indisposition, stress etc.
All of that is something I had to live with for a long time. The investigations made on me always resulted in palliative measures that mitigated the problem for a short time.
I passed through implants and placement of prostheses which even without having (those measurements) the aim of healing this malaise I still had the hope that it would: but the relief only worked for a short period of time. Finally, by indication of my dentist, I arrived at Clinic MY starting then the TMJ treatment. Shortly after the start of the treatment the symptoms started to fade.
I am very thankful for the professionalism and dedication that I found there. Today, feeling better, I go back there for periodic evaluations and also to have the opportunity of thanking once more.”

You are singing my tune!
Example mid 30’s woman came with persistant whiplash pain after a fat woman fell on her. She had c/spine fusions (C2/3 and later C5/6).
As the pain persisted the surgeon place LA into Levator Scapulae. This stopped much of the pain – so the shoulder muscle was sectioned – leading to loss of sholulder control – dropped shoulder and brachial plexus stretching – Carpal Tunnel problems and loss of fine motor control. Unable to brush her teeth she presented at my clinic.
I made a corrective splint to enhance airway and decompress the TMJ’s.
3 years of high level (9/10) pain was essentially gone (3/10) pain in the week.
What you are saying is brilliant as it shows this stuff in action.
Dr David Zimmerman
Stanmore Bay Dental
TMJ & Sleep Therapy Centre
ph +64 9 428 1081
LikeLike
Thank you David is good that we can help our patients. My best regards.
LikeLike
Amazing documentation and analysis. God Bless you Lidia for your dedication to help these complicated cases 💐.
LikeLike
Thank you Dr. Prafulla Thumati!
LikeLike