
57-year-old female patient attended the consultation in 2017 complaining of pain in the temporomandibular joints and limited mouth opening. According to the anamnesis completed by the patient herself at the initial consultation, she reports occasional headache, tinnitus, nonspecific facial pain, strange sounds in both ears, difficulty in opening her mouth and pain in both TMJs (temporomandibular joints).
The patient reports that her symptoms started in 2011 after a procedure to replace all old amalgam fillings with resins.
Brief report written by the patient
Dear Dr. Lidia,
Here is the succinct account of what happened to my maxilar or jaw.
In 2011 I went to the dentist at the recommendation of a friend to remove the old fillings (amalgams).
The work was long during this year and I was satisfied with the result.
Months later the right side of my mouth started to bother me because I felt as if a gap was occurring when I closed my mouth. I returned to the professional and he again aligned the height of the teeth and improved a little.
I started to feel pain and in 2012 I was recommended to have a consultation with a professional specialist in TMD who prescribed Mioflex for pain.
I used a bruxism splint because I couldn’t open my mouth wide, it opened a little (it hurt the right side of my face)
 Postural front and back photographs of the patient at the first consultation in 2017.
Postural front and back photographs of the patient at the first consultation in 2017.
Shoulder misalignment and forward head posture.
 Postural photographs of the patient’s right and left profile at the first consultation in 2017.
Postural photographs of the patient’s right and left profile at the first consultation in 2017.
Important postural anteriorization of the head. Note the prognata profile.
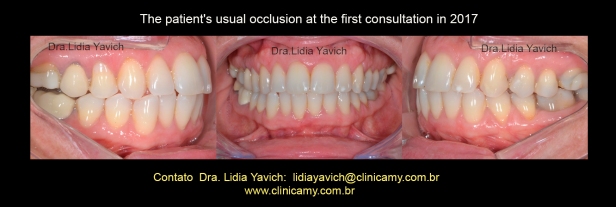 The patient’s habitual occlusion at the first consultation in 2017.
The patient’s habitual occlusion at the first consultation in 2017.
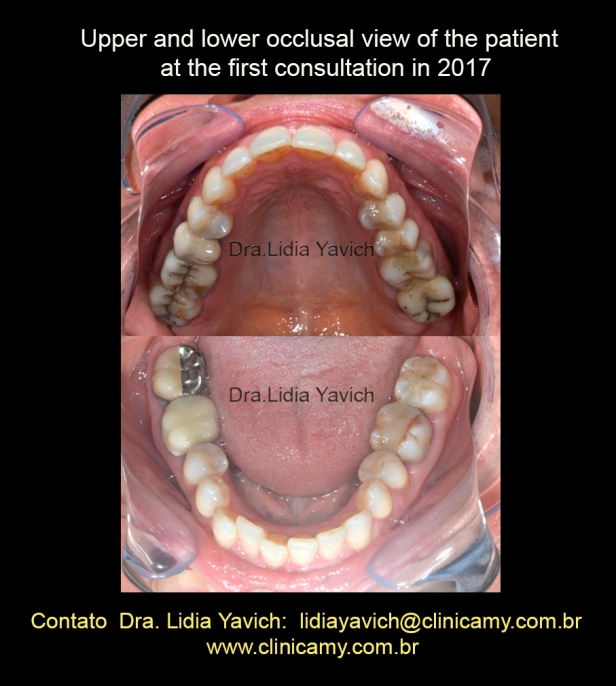 Upper and lower occlusal view of the patient at the first consultation in 2017.
Upper and lower occlusal view of the patient at the first consultation in 2017.
Small crowding in the lower incisor sector.
Continuation of the summary report written by the patient
After using the bruxism splint, the TMD specialist suggested physiotherapy with an excellent professional physiotherapist specialized in facial trauma with car accidents, etc.
With her consultations, the mouth returned to the place and the pain diminished a lot, but with the cold it pulled to the right again.
I took Mioflex boxes because it hurt me in the right TMJ region and gave me a headache.
I consulted more other orthodontists and recommended splints.
To relieve the pain I did more than a year of acupuncture with another physiotherapist. It was great because because the pain relieved a lot. The physiotherapist left to live outside Brazil and I didn’t do acupuncture anymore
One day in 2017 having a lot of pain I found your name on the internet and read a wonderful testimony.
I went to see you, but I was unable to do the treatment.
 Panoramic radiograph of the patient at the first consultation in 2017.
Panoramic radiograph of the patient at the first consultation in 2017.
 Laminography of the patient at the first consultation in 2017.
Laminography of the patient at the first consultation in 2017.
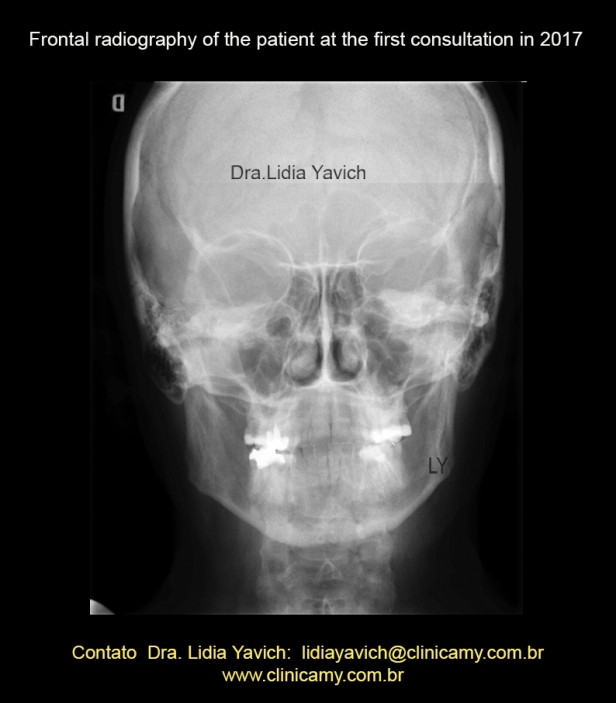 Frontal radiography of the patient at the first consultation in 2017.
Frontal radiography of the patient at the first consultation in 2017.
Mandibular deviation to the right.
Midline deviation to the right.
Cervical spine and odontoid process are centralized.
 Frontal radiography of the patient at the first consultation in 2017.
Frontal radiography of the patient at the first consultation in 2017.
Mandibular deviation to the right.
Midline deviation to the right.
Cervical spine and odontoid process are centralized.
Ilustration to facilitate the recognition of structures.
 Lateral radiography of the patient at the first consultation in 2017.
Lateral radiography of the patient at the first consultation in 2017.
The profile with mandibular protrusion is observed.
Important forward head posture.
 Lateral and cervical spine radiography of the patient at the first consultation in 2017.
Lateral and cervical spine radiography of the patient at the first consultation in 2017.
Important forward head posture.
The profile with mandibular protrusion is observed.
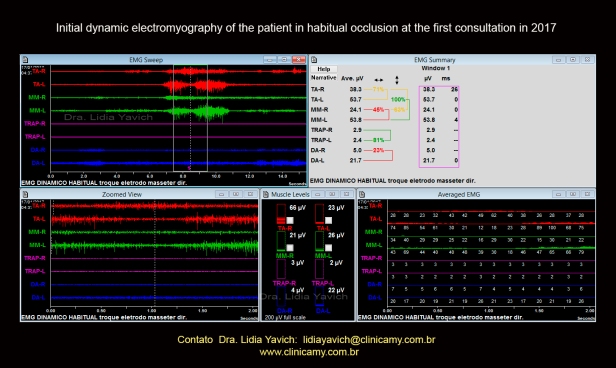
Initial dynamic electromyography of the patient in habitual occlusion at the first consultation in 2017.
This electromyography recorded in the consultation of the year 2017 shows significant asymmetry of the right and left temporal muscles between each other also asymmetry between the right and the left masseter. Right masseter spasm with very little activation at maximum intercuspation. The digastric muscle on the left side in constant activation during all functions.
In this electromyography, the patient is asked to open and close her mouth. Clench the teeth tightly at maximum intercuspation and swallow.
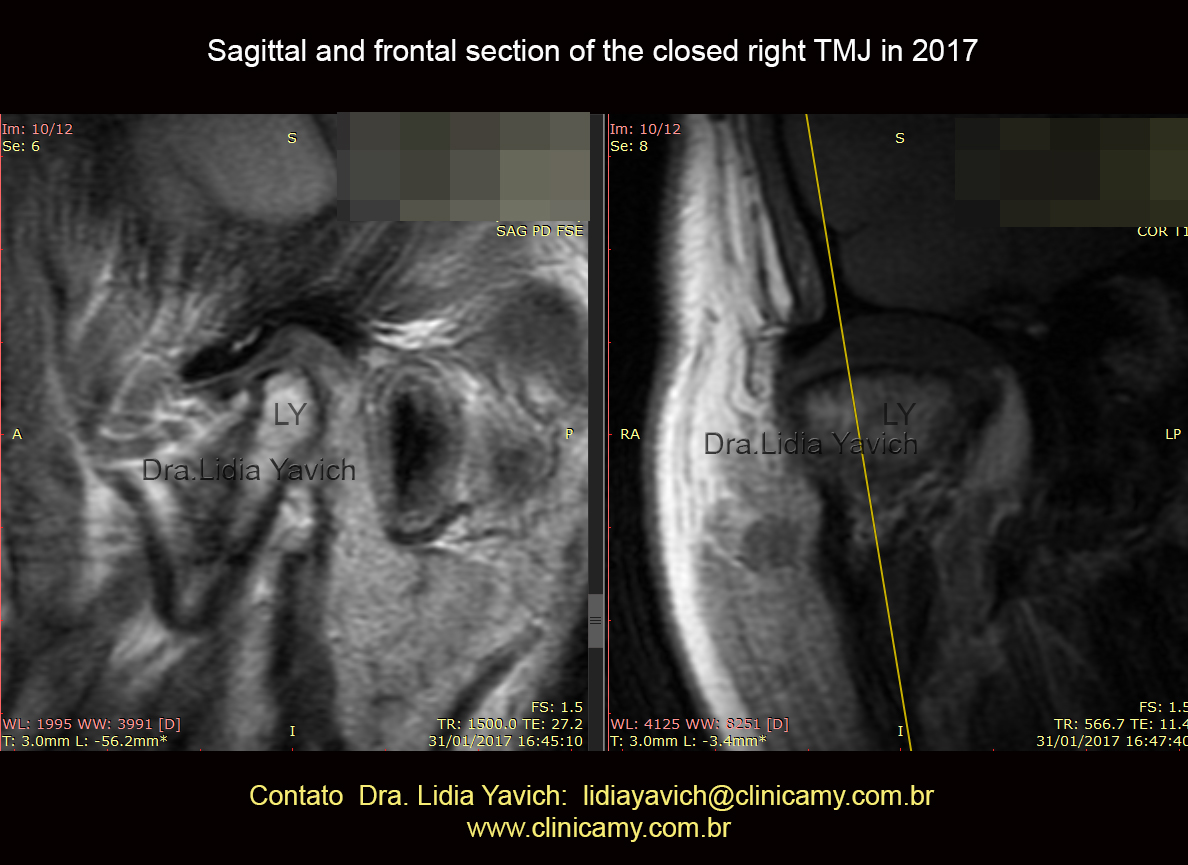 MRI: DP sagittal and T1 frontal view of the closed right TMJ in 2017.
MRI: DP sagittal and T1 frontal view of the closed right TMJ in 2017.
Deflection of the mandibular condyle due to trauma in early childhoodand rectification of the upper aspect of the mandibular condyle.
 MRI: DP sagittal and T1 frontal view of the closed left TMJ in 2017.
MRI: DP sagittal and T1 frontal view of the closed left TMJ in 2017.
The image is not good due to the patient’s nervousness inside the resonator. The mandibular condyle on the left side is anteriorized even with the mouth closed.
 MRI: T1 sagittal section of both right and left TMJs open mouth in 2017.
MRI: T1 sagittal section of both right and left TMJs open mouth in 2017.
The limitation of opening of the right condyle can be observed, coinciding with the clinical complaint. In this image, we can observe the sequela of a green fracture in the right condyle due to trauma in early childhood.
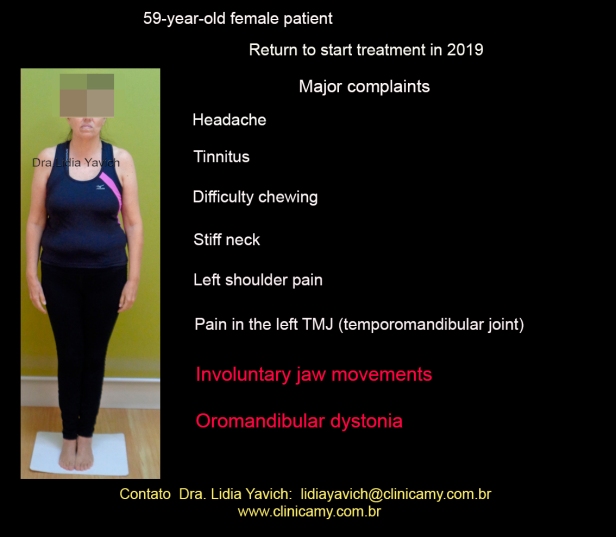 The same 59-year-old female patient returns to consult to start the treatment in 2019, two years after the first consultation. According to the anamnesis, again filled out by the patient herself at the consultation, she reports: occasional headache, tinnitus, difficulty in chewing, stiff neck, pain in the left shoulder, pain in the right TMJ. Involuntary movements of the mandible, Oromandibular Dystonia.
The same 59-year-old female patient returns to consult to start the treatment in 2019, two years after the first consultation. According to the anamnesis, again filled out by the patient herself at the consultation, she reports: occasional headache, tinnitus, difficulty in chewing, stiff neck, pain in the left shoulder, pain in the right TMJ. Involuntary movements of the mandible, Oromandibular Dystonia.
Dystonia and oromandibular dystonia
Dystonia can be defined as involuntary and prolonged contractions, resulting in twisting movements and the adoption of abnormal positions. Involuntary rhythmic and oscillatory movements, due to alternating or synchronous contraction of antagonistic muscles with reciprocal innervation.
Dystonia can occur practically in all muscle groups. Various names are used to describe the different locations of dystonia.
Oromandibular dystonia is called when it is located in the lower part of the face, lips and jaw, the patient presenting involuntary closing of the mouth opening, retraction or pursing of the lips and may present repeated contractions of the platysma.
Summary report written by the patient on return for treatment in 2019, continuation of the report in 2017 at the first consultation.
After consulting with you in 2017, I was appointed at the time to another professional and soon put on the first functional device. The pain disappeared and the mouth started to return to its normal position (it pulled a lot to the right).
I used two more devices with her always mobile, the last one showing improvement in the symmetry of my face.
She did what she can up to here and now I’m following you, because I want my smile back and also the tinnitus to disappear.
When I take Frontal night (alprazolam) my facial muscle relaxes and the jaw returns to its normal position, but when the effect passes the jaw starts to shift again.
I also use this last device at night that the professional that was treating me made.
It is important to say that I have been to two neurologists and the observation was for me to always control vitamin B12 Since the first consultation I have been taking Citoneurin.
Trauma history:
In 1996 I don’t remember the year well, I fell off a stair and I hit my back until I hit the floor. I was seen at the hospital and had no fractures.
In 2003 I had an accident at an amusement park when a stroller that came behind mine, without brakes hit my back violently.
I was treated at the hospital, there were no fractures, I wore a vest around my neck for a while and I took Tramal.
I suffered two more car accidents where they hit me in the back and I suffered what is called “whiplash” I was driving.
I work weight training twice a week since two years ago, before I did Pilates.
As far as I know I have one leg shorter than the other.
Documentation of the patient when she returned in 2019, to start treatment
 Postural front and back photographs of the patient when she returned to start treatment in 2019.
Postural front and back photographs of the patient when she returned to start treatment in 2019.
It is noteworthy the mandibular deviation to the right in comparison with the postural photographs of the year 2017, which will be compared later on.
 Postural photographs of the patient’s right and left profile when she returned to start treatment in 2019.
Postural photographs of the patient’s right and left profile when she returned to start treatment in 2019.
It is noteworthy that the jaw that had a protruded position in the first photographs shows a more straight position compared to the postural photographs of the year 2017, which will be compared further ahead.
Video of the patient at the consultation in 2019 when she returns using a functional device, which relieved certain pains, but already with OROMANDIBULAR DYSTONIA.
Note the patient’s difficulty in closing her mouth.
A filter was placed in the eyes to not identify the patient . The patient tries to close her eyes tightly to control the mandibular movement (sensory trick), but fails.
 Patient’s habitual occlusion when she returned to start treatment in 2019.
Patient’s habitual occlusion when she returned to start treatment in 2019.
It is noteworthy a modification of the median line in comparison with the postural photographs of the year 2017, which will be compared later
 Upper and lower occlusal view of the patient when she returned to start the treatment in 2019.
Upper and lower occlusal view of the patient when she returned to start the treatment in 2019.
Draws attention, the alignment of the lower crowding in comparison with the occlusal photographs of the year 2017, which will be compared later.
 Panoramic radiograph of the patient when she returned to start treatment in 2019.
Panoramic radiograph of the patient when she returned to start treatment in 2019.
 Laminography of the patient when she returned to start treatment in 2019.
Laminography of the patient when she returned to start treatment in 2019.
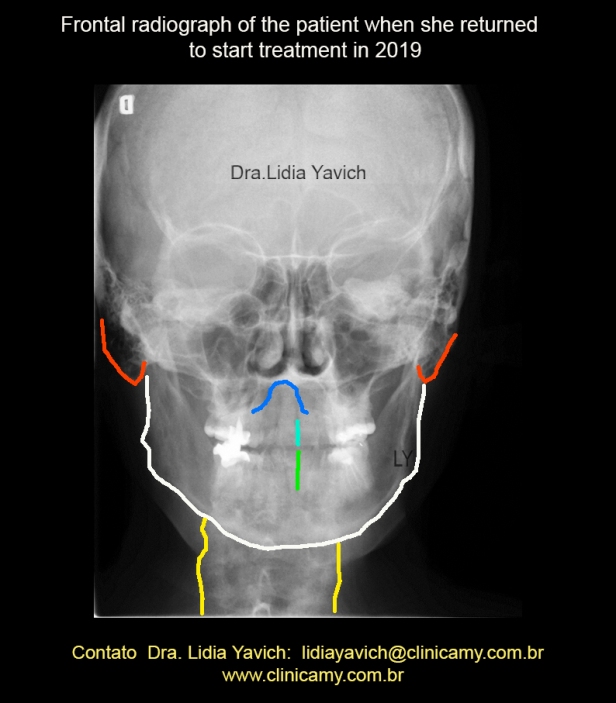
 Frontal radiography of the patient when she returned to start treatment in 2019. Important lateralization of the cervical spine to the right and sliding of the odontoid process of the axis to the right compared to the frontal radiography of the year 2017, which will be compared later on.
Frontal radiography of the patient when she returned to start treatment in 2019. Important lateralization of the cervical spine to the right and sliding of the odontoid process of the axis to the right compared to the frontal radiography of the year 2017, which will be compared later on.
 Frontal radiography of the patient when she returned to start treatment in 2019. Important lateralization of the cervical spine to the right and sliding of the odontoid process of the axis to the right compared to the frontal radiography of the year 2017, which will be compared later on.
Frontal radiography of the patient when she returned to start treatment in 2019. Important lateralization of the cervical spine to the right and sliding of the odontoid process of the axis to the right compared to the frontal radiography of the year 2017, which will be compared later on.
Design to facilitate recognition of structures.
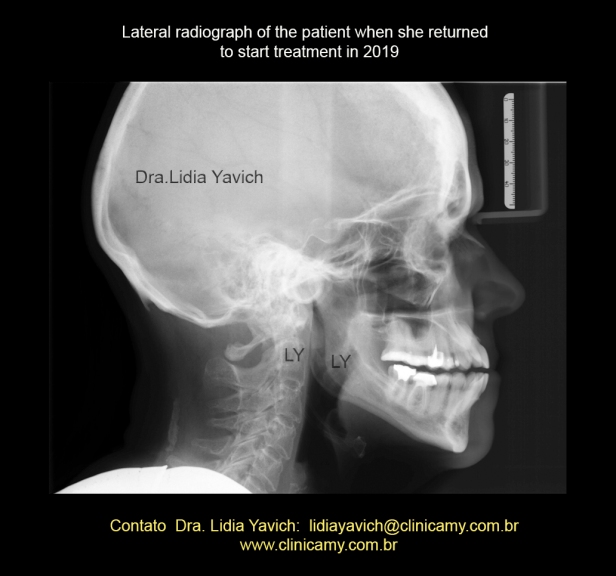 Lateral radiograph of the patient when she returned to start treatment in 2019.
Lateral radiograph of the patient when she returned to start treatment in 2019.
It is noteworthy that the jaw that had a protruded position on the first radiographs presents a more straight position compared to postural photographs from the year 2017, which will be compared later on.

Lateral and cervical spine radiography of the patient when she returned to start treatment in 2019.
It is noteworthy that the jaw that had a protruded position on the first radiographs presents a more straight position compared to postural photographs from the year 2017, which will be compared later on.
Increased upper thoracic kyphosis and anteriorization of the sixth cervical vertebra compared to the X-rays of the year 2017, which will be compared later.
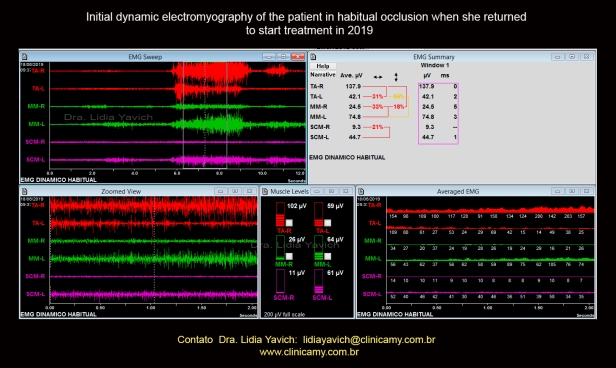 This dynamic electromyography recorded in the consultation of the year 2019 shows greater asymmetry of the right and left masseter pairs muscles between them and the right and left temporal muscles between them, compared to the electromyography recorded in the year 2017.
This dynamic electromyography recorded in the consultation of the year 2019 shows greater asymmetry of the right and left masseter pairs muscles between them and the right and left temporal muscles between them, compared to the electromyography recorded in the year 2017.
The right masseter muscle is in spasm with very low activation at maximum intercuspation. In this electromyography, the right and left sternocleidomastoids were measured. The sternocleidomastoid muscle on the left side is activated during all functions.
 MRI: T1 sagittal section of both right and left open TMJs when the patient returned to start the treatment in 2019.
MRI: T1 sagittal section of both right and left open TMJs when the patient returned to start the treatment in 2019.
The right condyle improved the opening but is still limited. The right mandibular head has a deflection and gives an appearance that comes to eminence. The opening in cases with deflection should be evaluated with reference to the continuation of the body and mandibular neck. In this image, the sequela of a green stick fracture due to trauma in early childhood can be observed very well in the right condyle.
 MRI: Sagittal and frontal slice of the right TMJ closed mouth when the patient returned to start treatment in 2019.
MRI: Sagittal and frontal slice of the right TMJ closed mouth when the patient returned to start treatment in 2019.
Slight retroposition of the condyle in the sagittal section compared to the 2017 image.
 MRI: Sagittal and frontal view of the left TMJ closed mouth when the patient returned to start treatment in 2019.
MRI: Sagittal and frontal view of the left TMJ closed mouth when the patient returned to start treatment in 2019.
Retroposition of the condyle in the sagittal section compared to the 2017 image where it was in more forward position.
Comparison of the patient’s documentation of the first consultation in 2017 and when she returned to start treatment in 2019.
 Comparative frontal images of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Comparative frontal images of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Note the greater mandibular deviation to the right compared to the postural photographs of 2017.
Greater forward-rotation of both shoulders.
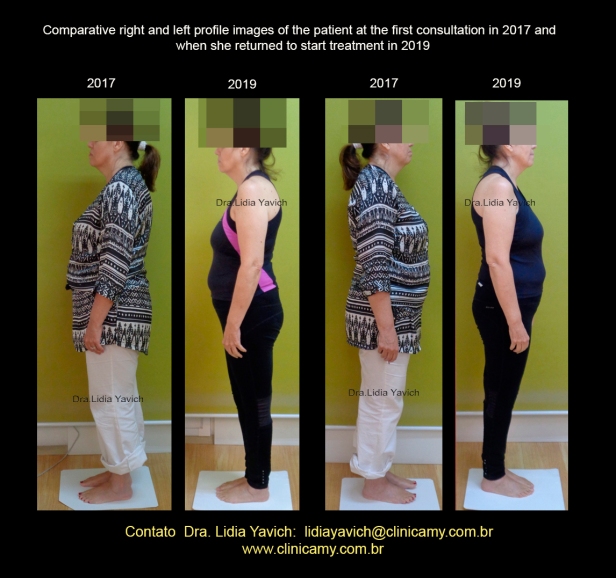 Comparative right and left profile images of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Comparative right and left profile images of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Greater forward-rotation of both shoulders in 2019 images
Increased forward posture of the head in the 2019 images even more displacing the center of gravity.
The jaw is more retro positioned in the images of 2019 compared to the images in 2017.
 Comparative images of the patient’s habitual occlusion when she returned to start treatment in 2019.
Comparative images of the patient’s habitual occlusion when she returned to start treatment in 2019.
Modification of the median line compared to postural photographs from the year 2017.
 Comparative images of the patient’s upper and lower occlusal view when she returned to start treatment in 2019. The alignment of the lower crowding in comparison with the occlusal photographs of the year 2017 is noteworthy.
Comparative images of the patient’s upper and lower occlusal view when she returned to start treatment in 2019. The alignment of the lower crowding in comparison with the occlusal photographs of the year 2017 is noteworthy.
 Comparative frontal radiographs of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Comparative frontal radiographs of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Important lateralization of the cervical spine to the right and sliding of the odontoid process of the axis to the right compared to the frontal radiography of the year 2017.
 Comparative frontal radiographs of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Comparative frontal radiographs of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Important lateralization of the cervical spine to the right and sliding of the odontoid process of the axis to the right compared to the frontal radiography of the year 2017. Design for easy viewing.
 Comparative lateral radiographs of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Comparative lateral radiographs of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
The jaw that had a protruded position on the first radiographs shows a straighter position compared to postural photographs from the year 2017. A more compressed position.
Greater forward posture of the head on the 2019 radiography compared to the 2017 radiography.
 Comparative lateral and cervical spine radiographs of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
Comparative lateral and cervical spine radiographs of the patient at the first consultation in 2017 and when she returned to start treatment in 2019.
The jaw that had a protruded position on the first radiographs shows a straighter position compared to postural photographs from the year 2017. A more compressed position.
Greater forward posture of the head on the 2019 radiography compared to the 2017 radiography.
Increased high thoracic kyphosis on the 2019 radiography compared to the 2017 radiography.
Video of the patient when she returned for treatment BEFORE placing the orthotic on her.
You can notice the involuntary movement of the jaw and the patient trying to press her lips to control the movement.
A filter has been placed and the audio is removed.
Video Content: Good morning, what you have is an oromandibular dystonia, did you know that?
The Dr. who was treating me took my case to São Paulo, at a congress and commented on oromandibular dystonia. Then I consulted with a neurologist who said it was dyskinesia. He claimed that MRI showed nothing that neurologically I had nothing. He said he could continue with the functional device and prescribed an anxiolytic and Citoneurin.
Initiation of the treatment:
In this specific case of oromandibular dystonia, IT WAS NOT POSSIBLE to use a computerized jaw tracker to record the bite, due to lateral mandibular movements.
 It was not possible to record the neuromuscular physiological rest position of the mandible with the jaw tracker, invalidated due to the involuntary movements of the patient’s jaw.
It was not possible to record the neuromuscular physiological rest position of the mandible with the jaw tracker, invalidated due to the involuntary movements of the patient’s jaw.
 Example of a record with the jaw tracker in a physiological neuromuscular rest position of a patient with TMJ pathology, but WITHOUT OROMANDIBULAR DYSTONIA. We can observe the symmetrical and repetitive pulse that corresponds to the elevation of the mandible by the action of TENS.
Example of a record with the jaw tracker in a physiological neuromuscular rest position of a patient with TMJ pathology, but WITHOUT OROMANDIBULAR DYSTONIA. We can observe the symmetrical and repetitive pulse that corresponds to the elevation of the mandible by the action of TENS.
The bite registration for the construction of the orthotic was performed using information from the surface electromyography (record already posted) and Tens, without using the jaw tracker due to mandibular movements. Taking into account joint decompression and manual muscle tests of arms and legs strength in coordination with the orthotic.
Together with the installation of the orthotic for continuous use, the patient was referred for osteopathic treatment with Dr. Kaciane Boschetti to adjust the biomechanics and body alignment.
Video with the patient wearing the mandibular orthotic.
A filter has been placed and the audio is removed.
Video Content:
Hi, how are you?
Hi Dr. Good morning on this wonderful day full of the warmest spring sun, I am here very happy doing my review.
My mouth, the jaw is getting back to normal, this rush that the jaw was doing, it is passing , I’m feeling very positive about the treatment, I know this is a walk I’ve been here for a while and I’m at least having my face back. I hope to be totally cured, I believe in miracles, but it doesn’t depend on me anymore. I’m doing what I have to do.
Video with the patient without the mandibular orthotic.
A filter has been placed and the audio is removed.
Video Content:
I am recording this video for you to tell you that I am going out to dinner now, I put on makeup, put on lipstick and I am hoping to be successful tonight.
I want to thank you for the affection and dedication with me. A big kiss dear. I have no device now.
Considerations of movement disorders and their connection to the TMJ.
Dystonia is a term that defines a group of diseases characterized by involuntary muscle spasms that generate abnormal movements and postures of a certain part or the whole body.
Oromandibular dystonia: is characterized by spasms in the lower region of the face, such as the lips, mouth, tongue and jaws. The most frequent symptoms are difficulty in chewing, opening the mouth, swallowing food and articulating words.
The prevalence of temporomandibular disorders in oromandibular dystonia is very high. It is important that health professionals are familiar with oromandibular dystonia and temporomandibular disorders.
The dental nerve that innervates the jaw muscles and the TMJ also mixes with the nerves in the neck. Therefore, dysfunction in the cervical structures usually leads to problems in the jaw and vice versa.
Neuritis of the auriculotemporal branch of the trigeminal nerve, which has a direct entry into the reticular formation (RF) can activate the cells in the pontine region of RF known for the control and deviation of the head posture.
Precision orthotics can help by modifying the nociceptive reflexes in the region of the temporomandibular joint. It is essential to work on biomechanical adjustments and body alignment carried out by specialized professionals with experience in dystonic patients.
Each patient is UNIQUE, the time and the result are also unique for each patient. In general, those patients where focal dystonia has been installed for a shorter time have a faster and more favorable response.
There are patients who take years to improve and others where the improvement is faster. You can’t predict this at the beginning.
In this specific case, the patient feels very well nowadays without the use of the orthotic this fact is unusual, my recommendations: always to take the orthosis with her and continue with all the indications given by the osteopath.
I asked the patient for radiographs to assess changes in both the mandible and the upper cervical.
I am deeply grateful to Dr. Anthony B. Sims for his teachings in the area of movement disorders and its relationship with the TMJ.
This knowledge is essential due to the large number of patients who can be helped.
Testimony of the patient:
 Good night Dr. Lidia
Good night Dr. Lidia
Follow my testimony.
These past few months have been wonderful in my life.
In 2011, when changing the old amalgam of my teeth, I entered a year later in a journey of intense pain on the right side of my face, in addition to having a very strong drawing of my jaw in this same direction.
Even using a functional appliance, my condition worsened until I received a diagnosis of oromandibular dystonia.
There were many dentists and doctors that I consulted but the improvement started to happen with the treatment suggested by Dr. Lidia with the use of a splint totally different from the ones I had used previously.
During the first consultations I was fully evaluated considering my movements and posture.
Thanks to God through this new protocol that I tried I started to feel relevant improvements the pain started to decrease a lot.
During this period I totally changed my physical exercises and started dancing and walking a lot too (advice from the osteopath Dr. Kaciane Boschetti indicated by Dr. Lidia).
I started to have more health and also looked for a more nutritious diet because I had a low immunity during this period.
Today I take supplements including higher doses of vitamin D, magnesium chloride for anxiety control. I also have permanent control of the B and C complex vitamins as well as type 2 collagen which had a direct effect on pain relief.
With the continued use of the orthotic the jaw started to return to the place and this was a real miracle!
The movement on the right side of the face no longer exists.
I believe that the neurological system has absorbed the new position of the face and the alignment of the face has improved.
It was just a few months and the result was surprising.

I have no more pain. I can chew any food without difficulty and speak normally without the jaw pulling.
After the entire period of treatment I find that I learned new principles of healthy health. Small initial jaw disorders if not treated properly can lead to dystonia!
My smile came back and I currently don’t use the orthotic anymore.
First of all, I thank God for life and for inspiring Dr. Lidia to study movement disorders in the face because it was through her knowledge that today I am cured.
A hug God bless
