
The patient of this post contacted me through a derivation from a colleague from abroad.
Soon after he sent an email where he explained the motif for his consultation on Cervical Dystonia or Spasmodic Torticollis, I answered that it was not my
knowledge area, that I treated TMJ Pathologies , Orthodontics and Facial Orthopedics.
The patient insisted, commenting that the colleague that recommended me and knew me from the AACP meeting where I was invited as a lecturer explained to him that he didn´t know if I treated Distonia, but he thought that considering what he had watched I could help him.
I began to study more on published articles of this field. One of the articles that impacted me was: Spasmodic Torticollis: The Dental Connection. Anthony b. Sims, D.D.S.; Brendan C> Stack, D>D>S> ;MS.;Gary Demererjian, D.D.S.

Dystonia is a neurological movement disorder, which sustained muscle contractions causing twisting and repetitive movements or abnormal postures. The movements may resemble a tremor. Dystonia is often initiated or worsened by voluntary movements, and symptoms may “overflow” into adjacent muscles.There are multiple types of dystonia, and numerous diseases and conditions may cause dystonia.
Focal dystonia: affects a muscle or group of muscles in a specific part of the body causing involuntary muscular contractions and abnormal postures, like eyes, neck or hands.The precise cause of primary dystonia is unknown .It is suspected to be caused by a pathology of the central nervous system, likely originating in those parts of the brain concerned with motor function, such as the basal ganglia.

Main common dystonia denomination are :
A blepharospasm (from Greek: blepharon, eyelid, and spasm, an uncontrolled muscle contraction), is any abnormal contraction or twitch of the eyelid.
Oromandibular dystonia is a form of focal dystonia affecting the mouth, jaw and tongue, and in this disease it is hard to speak.
Cervical dystonia (spasmodic torticollis ) affects the muscles of the neck. Causes the head to rotate to one side, to pull down towards the chest, or back, or a combination of these postures.
Spasmodic dysphonia (or laryngeal dystonia) is a voice disorder characterized by involuntary movements or spasms of one or more muscles of the larynx(vocal folds or voice box) during speech.
Patient Testimony
Everything began approximately after the placement of the lower implants.
One year after that, I began to feel uncomfortable.
I felt a back and neck stiffness, a strong weight in the back of the head and pain.
I began to make a lot of examination tests with neurologists, physical therapists, rheumatologists, orthopedists.
All of them followed the same line, saying that it could be a stress problem and fatigue.
Later I began to feel a twist movement in my neck towards the left. It was not so strong but I felt I had no control on my neck.
My neck always tried to rotate to the left, especially when I walked and when I tried to hold an object.
After doing physical therapy, chiropractic’s, acupuncture and all those techniques I began to research and finally consulted another neurologist who told me that I had CERVICAL DYSTONIA.
He asked for many exams to eliminate the possibility of being a trauma or other problem related to Wilson disease. That hypothesis was soon discarded.
I consulted another neurologist that confirmed the same diagnosis: CERVICAL DYSTONIA.
The neurologist initiated a treatment with Botox, to alleviate, and to relax some muscles, trapeziums, sternocleidomastoids and splenius. I was also oriented to have three applications of miorelaxants.
I began to investigate more on the subject and I found some videos about TMJ and some treatments with dental appliances.

Patient Testimony
The situation is very bad because doctors say: “is neurological”, we don’t know the etiology and it has no cure until today.
I believe all of this must have a relation with the implants, because I passed more than 30 years without these teeth, maybe the position of my mouth could have provoked some slow alteration that end up in this situation.
I’m not an specialist to affirm that this is the real situation, but I believe that it is worthy to investigate because there is the existence of written articles.
Moreover Dr. Anthony Sims, and other doctors in the dentistry field point for possible head and neck disturbance, motor coordination, Tourette disease or something like that, so many things connected with TMJ (temporomandibular joints) disorders.

Patient report: Detail of principal symptoms
Impossibility of head stabilization
Ringing ears
Ear compression sensation
Muscle spasm when I want to move the head down and to the right.
Noises in the vertebras in the back of the neck region, may be C1 and C2, but I am not sure and noises in the spine.
Noises in the TMJ, specially when yawn.

Patient’s panoramic radiograph before treatment.

Patient’s frontal radiograph where it is clearly seen the impossibility for straight posture of the head.

Patient’s initial laminography, in habitual occlusion where we can observe the retro position of both mandibular heads.

Patient’s initial lateral radiograph in habitual occlusion before treatment.

We can observe in this lateral radiograph and cervical spine radiograph the total lack of space between the ATLAS posterior arc and the Occipital base. I suspected adherences so I solicited a lateral radiograph in flexion.

In the Cervical Spine radiograph in flexion we can observe a REDUCED space between the ATLAS posterior arc and the base of the occipital. THE SPACE IS REDUCED, BUT EXISTS.

The MRI in closed mouth shows a small disc, superior facets in both mandibular condyles and bilateral retro discal compression. The patient has no limitation in opening the mouth and the discs are well situated on the mandibular heads when opening. I didn´t judge important to include the image of open mouth for this clinic case.
tHE 
The Semg dynamic record shows an important asymmetry between anterior right and left temporalis, low activity of both masseters muscles. The trapezius doesn’t show activity during mandibular closing, which is physiologically correct. Important activity from the digastrics muscles in closing movement, which is not physiologically correct.

The Semg dynamic record shows an important asymmetry between anterior right and left temporalis, low activity of both masseters muscles. The sternocleidomastoid muscles show activity during mandibular closing, which is NOT physiologically correct (the sternocleidomastoid muscle is not a masticatory muscle). Important activity from the digastrics muscles in closing movement, which is NOT physiologically correct.

His masticatory muscles were electronically deprogrammed with TENS (Transcutaneal Electronic Neural Stimulation). A jaw tracker then registered a neurophysiologic position from where an intraoral appliance was constructed and tested with SEMG (Surface Electromyography.) For this record we used the neurophysiologic technique.
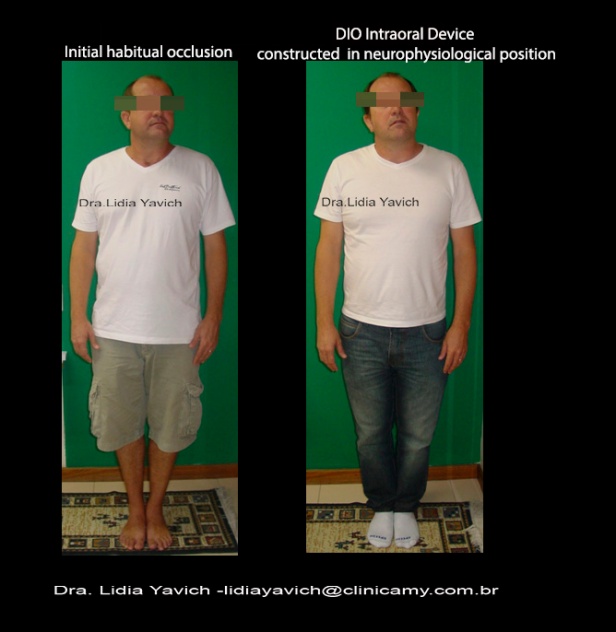
Patient’s frontal comparative images: initial and four months after DIO (Intra Oral Device) wear. Notice the important improvement of head and shoulder posture.

Patient’s right profile comparative images: initial and four months after DIO (Intra Oral Device) wear. Notice the important improvement of head and shoulder posture.
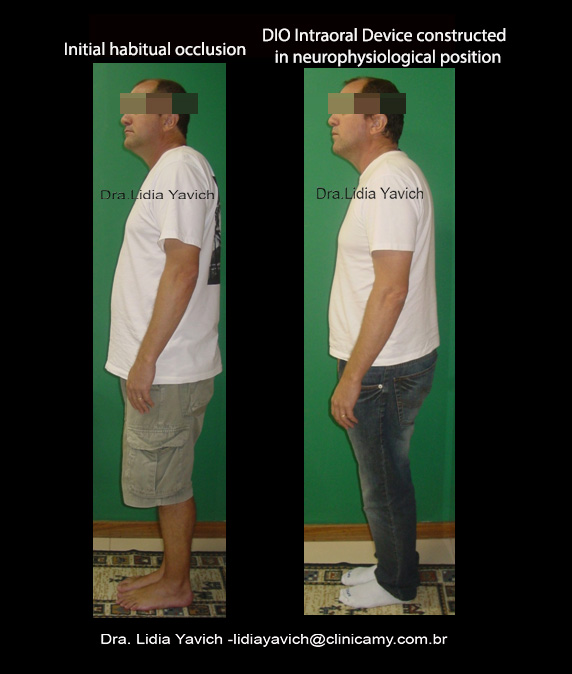
Patient’s left profile comparative images: initial and four months after DIO (Intra Oral Device) wear. Notice the important improvement of head and shoulder posture.

Patient’s lateral radiograph with the device in neurophysiological position. Notice the space between the posterior arc of the atlas and the occipital base that didn´t exist before.

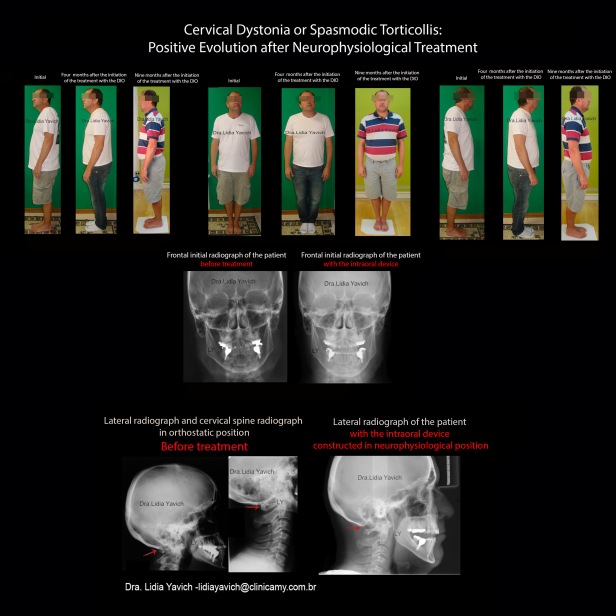
Patient’s frontal comparative radiograph: before the treatment and with the DIO (Intra Oral Device), the patient manages now to have a straight posture of the head.

Patient’s lateral and cervical spine comparative radiograph: before the treatment and with the DIO. Notice the space between the posterior arc of the Atlas and the occipital base that did not exist before.

Patient’s comparative laminographies: initial in habitual occlusion where we can observe the retro position of the mandibular heads and with the intraoral device with retrodiscal decompression.

Patient’s frontal comparative images: initial, four months and nine months after DIO wear. The patient had a physiological posture recovery.

Patient’s right profile comparative images: initial, four months and nine months after DIO wear. The patient had a physiological posture recovery.

Patient’s left profile comparative images: initial, four months and nine months after DIO wear. The patient had a physiological posture recovery.

Spasmodic Torticollis: The Dental Connection. Anthony b. Sims, D.D.S.; Brendan C> Stack, D>D>S> ;MS.;Gary Demererjian, D.D.S.
The patient also sent videos where he shows his initial incapacity to rotate the head and also comparative videos where he could do that again. The videos are not in the post to preserve patient’s identity.
