
Understanding the complex inter relation of craniomandibular disorders require a wide comprehension not only on anatomy and physiology of head and neck, but also of the vertebral spine. The cervical spine is the flexible link between the head and the trunk.
Only recently, dentistry began to think about the jaw and its association with the skull as a three-dimensional relationship, instead of considering it an isolated structure and evaluated in two dimensions as has been done traditionally.
To properly evaluate the maxillomandibular relationship we should start considering the physiological rest position.
Physiological rest is a concept, applicable to the rest of the body muscles
The stomathognatic muscles and not the exception

Male patient arrived to the clinic for consultation referring a strong pain behind the eyes, nonspecific facial pain, popping in the right temporomandibular joint and crackling on the same side.

The patient reports tingling and numbness in the cervical spine, tingling sensation in his right shoulder. He also reports pain and stiffness in the back of the neck, shoulder pain and muscular tremor.
The patient had completed an orthodontic treatment and after the removal of the orthodontic device he began to feel the reported symptoms .

Due to the strong symptoms the patient consulted several professionals: clinical dentist, physiotherapist, general practitioner and a orthopedist for the shoulder pain.
The orthodontist who treated him referred the patient to me, to see if I could help him.

Marking the pain points: headache, back of the neck stiffness, pain in the top of the head and in the forehead. Pain behind the eyes and in the back of the neck, popps, nonspecific facial pain, crepitus, dizziness and muscle tremor.
Patient’s habitual occlusion before treatment.

Patient’s occlusal superior and inferior view before treatment.
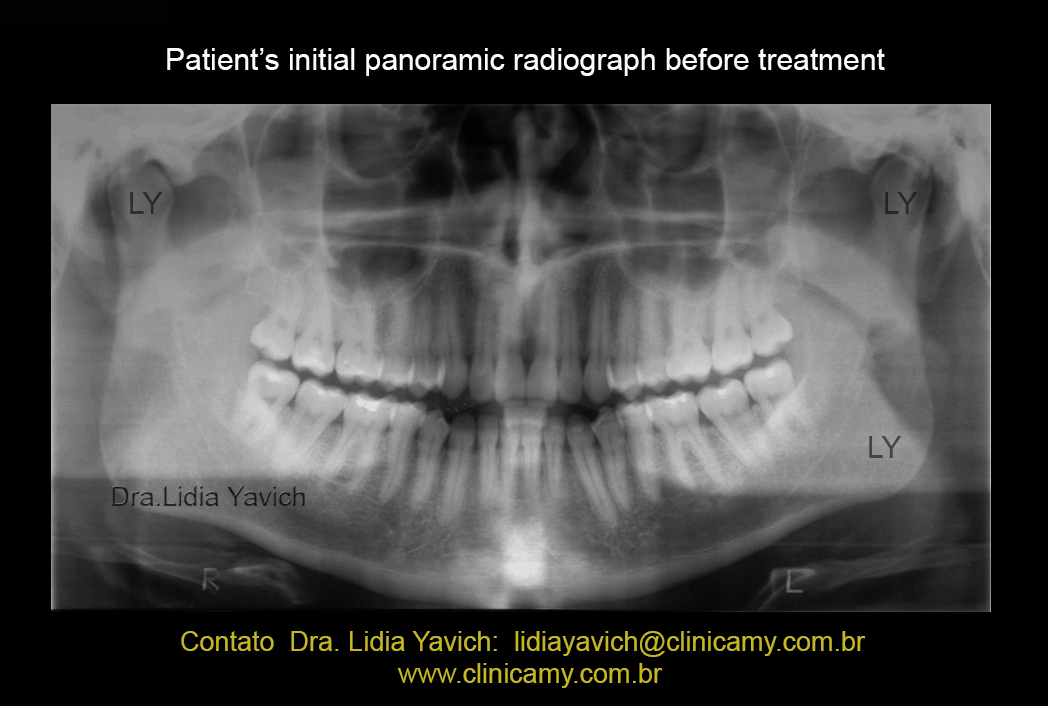
Patient’s initial panoramic radiograph before treatment.
 Patient’s TMJ right and left laminography, closed and open mouth before treatment.
Patient’s TMJ right and left laminography, closed and open mouth before treatment.
 Patient’s lateral radiograph before treatment.
Patient’s lateral radiograph before treatment.
 Patient’s frontal radiograph before treatment.
Patient’s frontal radiograph before treatment.
 Patient’s lateral radiograph and cervical spine before treatment.
Patient’s lateral radiograph and cervical spine before treatment.

Patient’s electromyography record in habitual occlusion before treatment.
In this dynamic record we registered the anterior right and left temporal muscles, the right and left masseter muscles, the right and left digastric muscles and the right and left upper trapezius muscles.
For this record we ask to the patient to open the mouth, close the mouth, clench strong and swallow.
Notice the asymmetry between the right masseter muscle and the left masseter muscle at maximal intercuspal sustained position. The digastric muscles during swallowing are activated before the masseter muscles which should not happen in a functional swallowing.

Patient’s initial kinesiographic record shows a significant loss of speed when the patient opens and closes the mouth. There is no coincidence between the neuromuscular trajectories in the sagittal view of the record.
The patient has hypermobile joints and has no limitation in opening the mouth.

MRI: sagittal slice left TMJ closed mouth. This image does not show significant alterations.

MRI: sagittal slice left TMJ closed mouth, this more medial slice shows the compression and the retroposition of the mandibular condyle. We can observe a facet on the top of the mandibular head.
REMEMBER THAT we are looking at a two-dimensional image and we have to understand that the COMPRESSION IS TRIDIMENSIONAL.

MRI: sagittal slice right TMJ closed mouth, this medial slice shows the compression and the retroposition of the mandibular condyle. We can observe a facet on the top of the mandibular head.
REMEMBER THAT we are looking at a two-dimensional image and we have to understand that the COMPRESSION IS TRIDIMENSIONAL.

MRI: sagittal slice right TMJ closed mouth, in this medial slice is even more evident the compression and the retroposition of the mandibular condyle. We can observe a facet on the top of the mandibular head.
REMEMBER THAT we are looking at a two-dimensional image and we have to understand that the COMPRESSION IS TRIDIMENSIONAL.

MRI: frontal slice from the right and left TMJ, closed mouth in habitual occlusion before treatment.
The right TMJ frontal slice makes clear a loss of joint space especially on the lateral pole.region In both frontal images we can notice the reduction of the joint space.

To properly evaluate the maxillomandibular relationship we should start considering the physiological mandibular rest position.
Physiological rest is a concept, applicable to the rest of the body muscles
The stomathognatic muscles and not the exception
The masticatory muscles of the patient were deprogrammed electronically and a new neurophysiological rest position was recorded.

With this data we constructed a DIO (intraoral device), to keep the three-dimensionally recorded position. This device must be tested electromyographically to objectively measure the patient.
Of course checking the patient’s symptoms is important, but the surface electromyography objectively shows if the muscular function improved, worst or did not change.
 Patient’s electromyographic record with the DIO (intraoral device), in neurophysiological position.
Patient’s electromyographic record with the DIO (intraoral device), in neurophysiological position.
Note the symmetry of the masseter muscles. The digastric muscles DON’T ACTIVATE before the masseter muscles during swallowing. This implies that the patient closes the teeth and swallows and not the contrary as the first record in habitual occlusion.

Patient’s kinesiographic record with the DIO (intraoral device): there has been an improvement in speed and COINCIDENCE in the trajectories when he opens and closes the mouth.

Patient’s frontal radiographs comparison: in habitual occlusion before treatment and with the DIO (intraoral device), in neurophysiological position.

Patient’s TMJ right and left closed and open mouth laminography comparison: in habitual occlusion before treatment and with the DIO (intraoral device), in neurophysiological position.

Patient’s lateral radiographs comparison: in habitual occlusion before treatment and with the DIO (intraoral device), in neurophysiological position.
In the middle of the treatment I referred the patient to a physical terapist for a postural reprogramming.
With the jaw in a neurophysiological position the physiotherapist colleague worked on the rest of the muscular chains. The patient also presented an incipient discopathy at the level of C3 and C6.

Patient’s panoramic radiograph comparison: before treatment and during the neurophysiological treatment.

Kinesiographic records comparison: in habitual occlusion before treatment and with the DIO (intraoral device), in neurophysiological position.
Note the improvement of the speed and the COINCIDENCE in the opening and closing trajectories.

Electromyography records comparison: in habitual occlusion before treatment and with the DIO (intraoral device), in neurophysiological position.
Note the symmetry of the masseter muscles, the digastric muscles DON’T ACTIVATE before the masseter muscles during swallowing. This implies that the patient closes the teeth and swallows and not the contrary as the first record in habitual occlusion before treatment.

The patient did not complained from pain and the other symptoms he had in the beginning of the treatment.The electromyography and kinesiographic records objectively showed the muscular function improvement.
We decided to start the SECOND PHASE of the treatment.
For this we used a three-dimensional orthodontics, where the teeth are erupted towards the new neurophysiological position. This procedure will allow us, following the technical steps to remove the DIO.

In the second phase, in this case the three-dimentional orthodontics the patient is monitored and electronically deprogrammed and many times the device is recalibrate to maintain the position obtained in the first phase.

Sequence of the second phase (in this specific clinical case).

Sequence of the second phase (in this specific clinical case).

Sequence of the second phase (in this specific clinical case).

Sequence of the second phase (in this specific clinical case).

Sequence of the second phase (in this specific clinical case).

Sequence of the second phase (in this specific clinical case).

Second phase completed!

Patient’s panoramic radiograph after the finalization of the three-dimensional orthodontics.

MRI: Comparison of the frontal section of the RIGHT TMJ closed mouth before neurophysiological treatment, and the same RIGHT TMJ closed mouth after the COMPLETION OF THE SECOND PHASE with the three-dimensional orthodontics.
Note the decompression of the temporomandibular joint, especially in the lateral pole.

MRI: Comparison of the frontal section of the RIGHT TMJ closed mouth before neurophysiological treatment, and the same RIGHT TMJ closed mouth after the COMPLETION OF THE SECOND PHASE with the three-dimensional orthodontics.
Note the decompression of the temporomandibular joint, especially in the lateral pole. Note the arrows.

MRI: Comparison of the frontal section of the LEFT TMJ closed mouth, before neurophysiological treatment, and the same LEFT TMJ closed mouth after the COMPLETION OF THE SECOND PHASE with the three-dimensional orthodontics.
Note the decompression of the temporomandibular joint.

MRI: Comparison of the frontal section of the LEFT TMJ closed mouth, before neurophysiological treatment, and the same LEFT TMJ closed mouth after the COMPLETION OF THE SECOND PHASE with the three-dimensional orthodontics.
Note the decompression of the temporomandibular joint. Note the arrows.

MRI: Comparison of the sagittal section of the LEFT TMJ closed mouth, before neurophysiological treatment, and the same LEFT TMJ closed mouth after the COMPLETION OF THE SECOND PHASE with the three-dimensional orthodontics.
Note the decompression of the temporomandibular joint.

MRI: Comparison of the sagittal section of the LEFT TMJ closed mouth, before neurophysiological treatment, and the same LEFT TMJ closed mouth after the COMPLETION OF THE SECOND PHASE with the three-dimensional orthodontics.
Note the decompression of the temporomandibular joint.

MRI: Comparison of the sagittal section of the RIGHT TMJ closed mouth, before neurophysiological treatment, and the same RIGHT TMJ closed mouth after the COMPLETION OF THE SECOND PHASE with the three-dimensional orthodontics.
Note the decompression of the temporomandibular joint.
Improvement in the relationship between the mandibular condyle and the articular disk.

MRI: Comparison of the sagittal section of the RIGHT TMJ closed mouth, before neurophysiological treatment, and the same RIGHT TMJ closed mouth after the COMPLETION OF THE SECOND PHASE with the three-dimensional orthodontics.
Note the decompression of the temporomandibular joint.
Improvement in the relationship between the mandibular condyle and the articular disk.

Patient’s electromyography record in neurophysiological occlusion AFTER THE FINALIZATION OF THE THREE DIMENSIONAL ORTHODONTICS.
Note the symmetry of the masseter muscles.
The digastric muscles DO NOT ACTIVATE before the masseter muscles during swallowing. This implies that the patient closes the teeth and swallows and not the contrary as the first record in habitual occlusion before treatment..
This means that the objectives achieved in the FIRST PHASE with the DIO in neurophysiological position were held after the finalization of the THREE DIMENSIONAL ORTHODONTICS.
 Patient’s electromyography records comparison:
Patient’s electromyography records comparison:
Before the treatment in habitual occlusion.
With the DIO (intraoral device), in neurophysiological position, during the FIRST PHASE of the treatment.
AFTER THE FINALIZATION OF THE THREE DIMENSIONAL ORTHODONTICS.

Patient’s lateral radiograph comparison:
Before the treatment in habitual occlusion.
With the DIO (intraoral device), in neurophysiological position, during the FIRST PHASE of the treatment.
AFTER THE FINALIZATION OF THE THREE DIMENSIONAL ORTHODONTICS.

Maxillomandibular values comparison:
Before the treatment in habitual occlusion.
With the DIO (intraoral device), in neurophysiological position, during the FIRST PHASE of the treatment.
AFTER THE FINALIZATION OF THE THREE DIMENSIONAL ORTHODONTICS.

In a recent revision after two years of completion of the SECOND PHASE with the three dimensional, I registered the habitual patient’s occlusion.
The patient continues free of symptoms.
In the postural mandible position and its complex three-dimensional relationship with the maxilla little details are essentials, especially in a hypermobile joint patient.
It is not a case of deep bite, not a case where simply moving the incisive guide anteriorly could solve the problem.
In the images the three-dimensional compression in this patient looks SUBTLE, but no less devastating.
Each case is different and every human being is a unique individual.

In the first evaluation, Dr. Lidia was very helpful explaining to me all the method of the treatment and what was necessary to achieve the expected results.
Along the way, I had neither more headaches nor joint pain, I was pain free.
Everyone in the team was very devoted to my treatment, and I had in the end an excellent result.
Today I am very grateful to Dr. Lidia and her team for all the attention.
Big huge to everyone from clinica my.

Would you be so kind to share your case? .
I would like to ask you some questions .
Thank you
LikeLike
Sure, you can send me an e-mail that is in the post or you can use lidiayavich@gmail .com
LikeLike